Eye Condition
Non-Arteritic Anterior Ischemic Optic Neuropathy (NAION)
NAION is a sudden optic-nerve “eye stroke” that can quickly steal vision; rapid integrative care at the Eye Health Institute may help preserve sight.
Explore our treatment options for Non-Arteritic Anterior Ischemic Optic Neuropathy (NAION)
What is NAION?
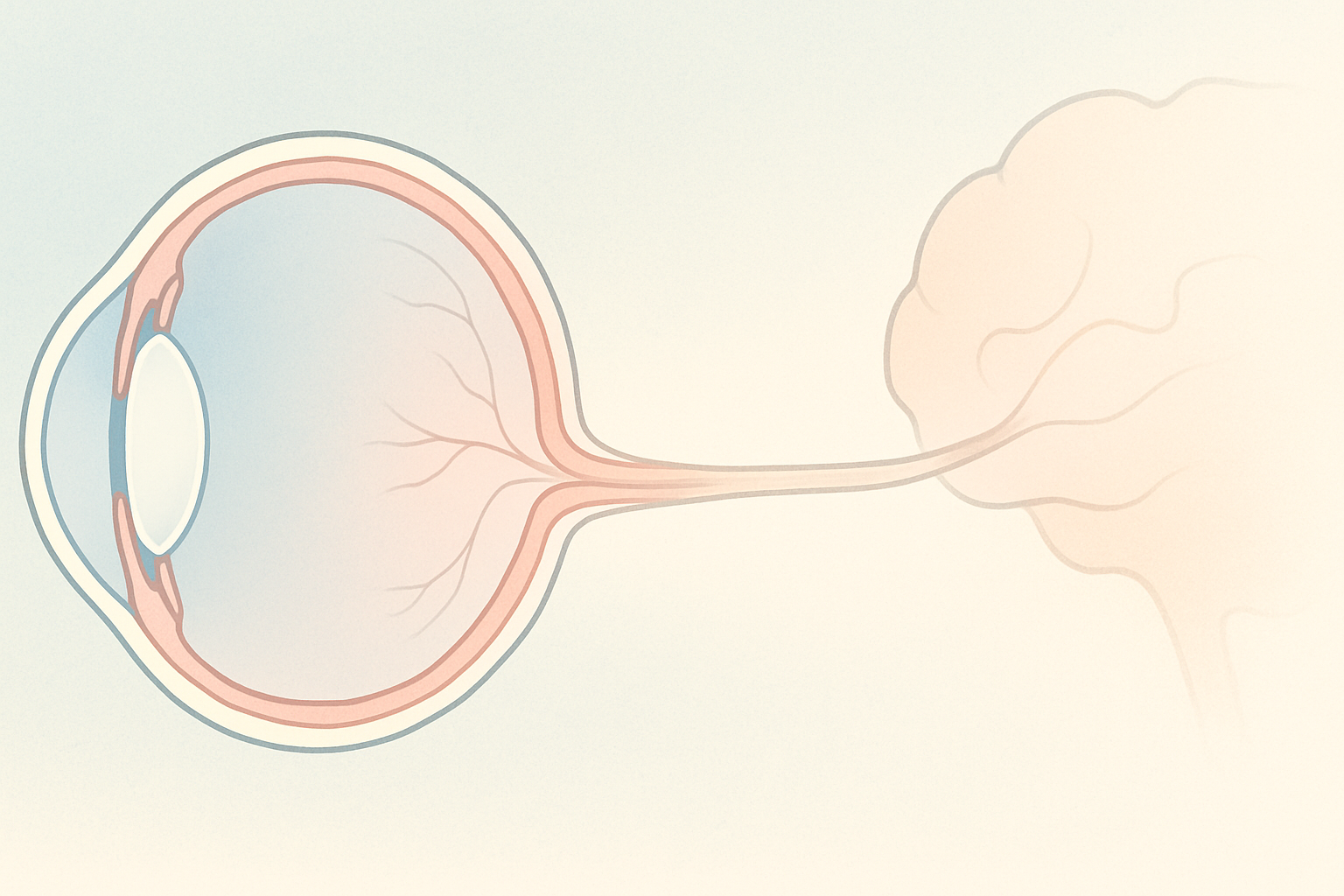
Non-arteritic anterior ischemic optic neuropathy (NAION) is an acute loss of blood flow (ischemia) to the front (anterior) of the optic nerve head. The swollen optic disc compresses tiny nerve fibers and vessels, disrupting the visual signal and causing patchy or profound vision loss—often overnight. NAION is the second-most common optic neuropathy after glaucoma and usually strikes adults over 50, though younger patients can be affected.
Key symptoms and early warning signs
- Sudden, painless vision dimming in one eye (rarely both), often noticed on waking
- Shadow or “curtain” in the upper or lower half of the visual field (altitudinal scotoma)
- Reduced contrast and color brightness
- Light fog or missing letters while reading
- Possible mild eye discomfort or headache around the brow
Because central reading vision can stay normal at first, many people ignore field loss until it worsens—timely testing is critical.
How NAION is diagnosed
Your eye doctor will:
- Dilate the pupil to inspect the optic nerve head for edema and pallor.
- Order visual-field testing to map scotomas.
- Perform optical coherence tomography (OCT) and fundus photography to document swelling.
- Check blood pressure, fasting glucose, cholesterol, and complete blood count.
- Rule out arteritic (giant cell) arteritis with ESR/CRP labs if symptoms suggest systemic inflammation.
Normal color vision and reading acuity do not rule out NAION; peripheral field testing is essential.
Why it happens: causes and risk factors
NAION arises when the small, crowded blood vessels that nourish the optic-nerve head lose perfusion. Contributing factors include:
- Pre-existing glaucoma or anatomically “disc-at-risk” small optic nerve heads
- Hypertension (≈50 % of cases)
- Type 1 or Type 2 diabetes (≈25 %)
- Obstructive sleep apnea requiring CPAP
- Hyperlipidemia, ischemic heart disease, or obesity
- Tobacco use or heavy alcohol intake
- Medications and stimulants that constrict vessels (erectile-dysfunction drugs, nasal decongestants, some arrhythmia drugs, cocaine, frequent energy drinks)
- Spikes in intraocular pressure or sudden blood-pressure drops at night
A single risk alone rarely causes NAION; it is the multiple hits of poor circulation, inflammation, and oxidative stress that tip the balance.
Conventional treatment options
Sadly, there is no proven pharmaceutical or surgical cure. Typical care may include:
- Short course of oral prednisone to shrink swelling
- Low-dose aspirin (≈100 mg daily) for platelet reduction
- Off-label anti-VEGF injections (bevacizumab, ranibizumab or aflibercept) – helpful for hemorrhage but often marginal for optic-disc edema
- Observation for six months, hoping partial vision returns (only about 40 % see modest improvement)
Because retinal tissue cannot survive prolonged hypoxia, the “wait and see” window can allow permanent axon loss.
Eye Health Institute’s integrative approach
Dr. Andy Rosenfarb emphasizes acting within days or weeks, treating NAION like an eye stroke. Our multimodal plan aims to restore oxygen, calm inflammation, and revive “sleeping” nerve cells:
| Therapy | Goal |
|---|---|
| Ophthalmic & Micro Acupuncture 48 | Dilate micro-capillaries, increase optic-nerve blood flow, speed lymphatic drainage of edema |
| Low-level laser acupuncture | Boost ATP and mitochondrial repair for damaged axons |
| Hyperbaric oxygen sessions | Saturate plasma with oxygen, counter acute hypoxia |
| Alternating-current stimulation (ACS-3000 home/clinic) | Re-activate dormant photoreceptor and ganglion pathways |
| Molecular hydrogen (H2) tablets or inhalation | Neutralize free radicals, temper oxidative stress |
| Targeted nutraceuticals | CBD-rich Catavision for inflammation, Total MA-48 for micro-circulation, neuronal support formulas, high-dose DHA, taurine, turmeric, ginkgo and ginger |
“If I see patients within a month of the episode, our recovery rate is very high because we can restore oxygen and wake up cells before they die.”
Care is individualized. We also coordinate with sleep specialists for untreated apnea, primary-care doctors for blood-pressure and lipid control, and teach home eye-qigong and stress-reduction practices.
What patients report and clinical insights
Many NAION clients arrive frustrated that they were told to “come back in six months.” In clinic we often observe:
- Disc edema shrinking faster—sometimes within two weeks—when acupuncture, laser and hyperbaric oxygen are combined.
- Visual-field plots showing reclaimed islands of sight after a series of ACS-3000 sessions.
- Reduced haze and sharper contrast once systemic inflammation falls (verified by CRP trends).
“Time is brain for the optic nerve—early circulation and anti-inflammatory work can mean the difference between a minor blind spot and permanent functional loss.”
Patients who adopt anti-inflammatory diets, consistent CPAP use, and gentle cardiovascular exercise maintain gains and lower the chance that the other eye will be struck. Integrative follow-up also screens for silent cardiovascular risks linked to NAION and more severe events such as retinal-occlusion eye strokes.

When to seek urgent care
Get urgent eye care now if you experience sudden vision dimming, a curtain-like shadow, worsening blind spot, new flashes with many floaters, severe eye pain, or any eye trauma. These may signal NAION, arteritic ischemic optic neuropathy, retinal detachment, or other emergencies requiring immediate evaluation.
Remember: NAION damage happens quickly, but so can support. Contact the Eye Health Institute or your nearest ophthalmologist at the first sign of vision change.