Best's Disease
Best’s disease, also known as Best’s vitelliform macular dystrophy, is a hereditary (usually) form of progressive macular dystrophy.
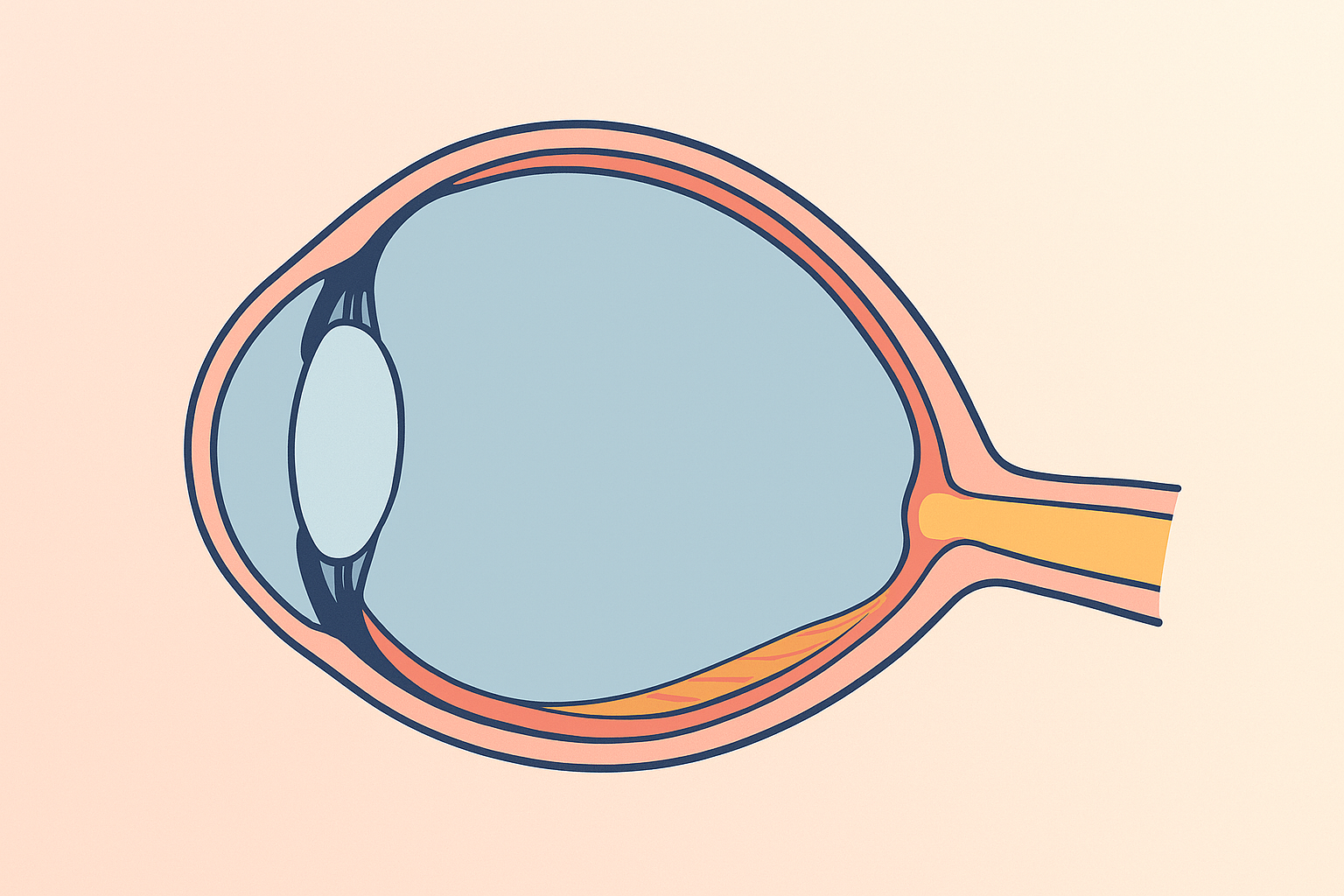
Central serous retinopathy is a condition that causes fluid to leak from the choroid layer into the macula, causing blurring or distortion of central vision.
Hear from Dr. Rosenfarb
Whether you prefer hands-on care, convenient telehealth visits, or self-guided learning, we have multiple ways to help you manage Central Serous Retinopathy.

Start here. A member of our care team will review your condition and situation, answer your questions, and walk you through the treatment options that are the best fit for you.
Book your free assessment call
Combining acupuncture, laser therapy & diagnostics at Dr. Rosenfarb's office in New Jersey. 90% of patients see measurable vision improvements.
Learn more
One-on-one virtual sessions with Dr. Rosenfarb. Get personalized assessment and custom treatment plan from home.
Learn more
Scientifically-formulated supplements chosen by Dr. Rosenfarb to nourish your eyes and support healthy vision recovery.
Get supplementsDr. Rosenfarb's top-recommended supplements to nourish and protect your eyes.

Supplements
$65.00

Vitamins & Supplements
$30.00

Supplements
$30.00$25.00
Save 17%

Eye Drops & Lubricants
$30.00
Ready to take the next step?
Choose whatever feels right for you — no pressure, no commitment.
Rated 5 stars by 10,000+ Happy Patients Worldwide
A real patient shares their journey with our treatment approach.
"I wish we would have found Dr. Rosenfarb and Acuvision sooner!"
This is what we hear from so many of our patients, like Ray and his wife, Lori. Ray (retinitis pigmentosa) and Lori (central serous retinopathy) drive 8 hours twice-yearly for micro-acupuncture, red-light and hydrogen therapies. Ray’s color and contrast sharpened after his first visit and have stayed stable for 12 years; Lori regained brightness in one week and left pain-free.
Common questions we get asked about Central Serous Retinopathy.
It shows up most often in healthy men between 20 and 50 years old, but women and older adults can be affected, especially if they have repeat or long‑lasting episodes.
High stress levels, steroid medications (pills, inhalers, creams, or bodybuilding hormones), high blood pressure, and sleep apnea all increase risk.
Sudden foggy or dim central vision, straight lines that look bent, colors that seem washed‑out, or a faint gray spot in the middle of what you see, all usually painless.
About four out of five first‑time cases dry up within three to four months without treatment, and most people regain nearly their previous level of clarity.
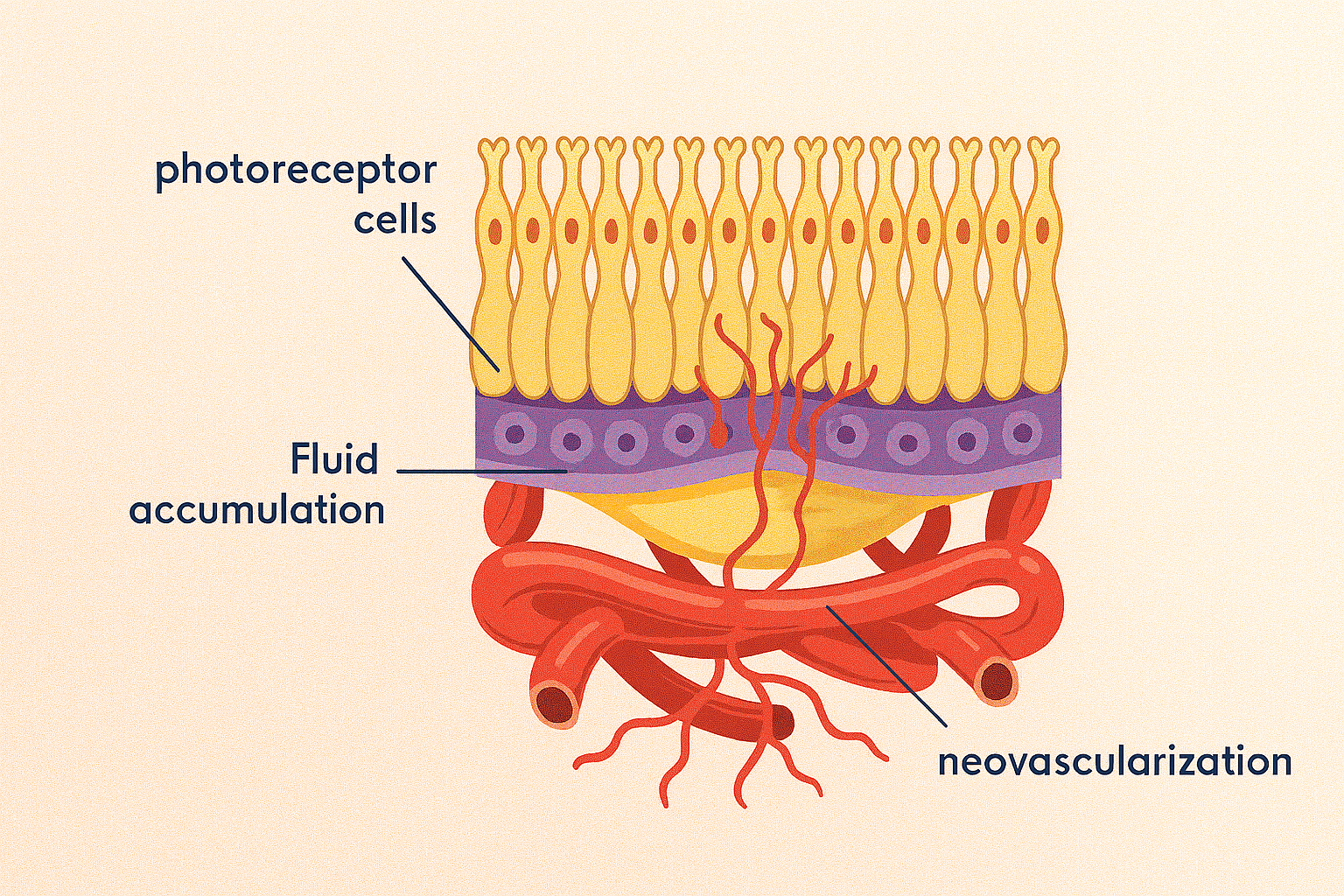
They rely on retinal imaging, especially OCT scans, to see the fluid blister, sometimes adding dye tests like fluorescein angiography to pinpoint the leak.
Persistent or recurrent pockets can damage retinal cells. In those cases doctors may use options such as low‑energy laser, photodynamic therapy, or medication to seal leaks and speed recovery.
If fluid drains quickly, eyesight often returns to 20/25 or better. Long‑standing detachments can leave mild, permanent drops in contrast or color perception.
Lowering stress, avoiding non‑essential steroid use, treating high blood pressure or sleep apnea, and having regular OCT check‑ups reduce the odds of another episode.
Discover other eye conditions that share similar causes, symptoms, or treatment approaches with the one you're exploring.
Best’s disease, also known as Best’s vitelliform macular dystrophy, is a hereditary (usually) form of progressive macular dystrophy.
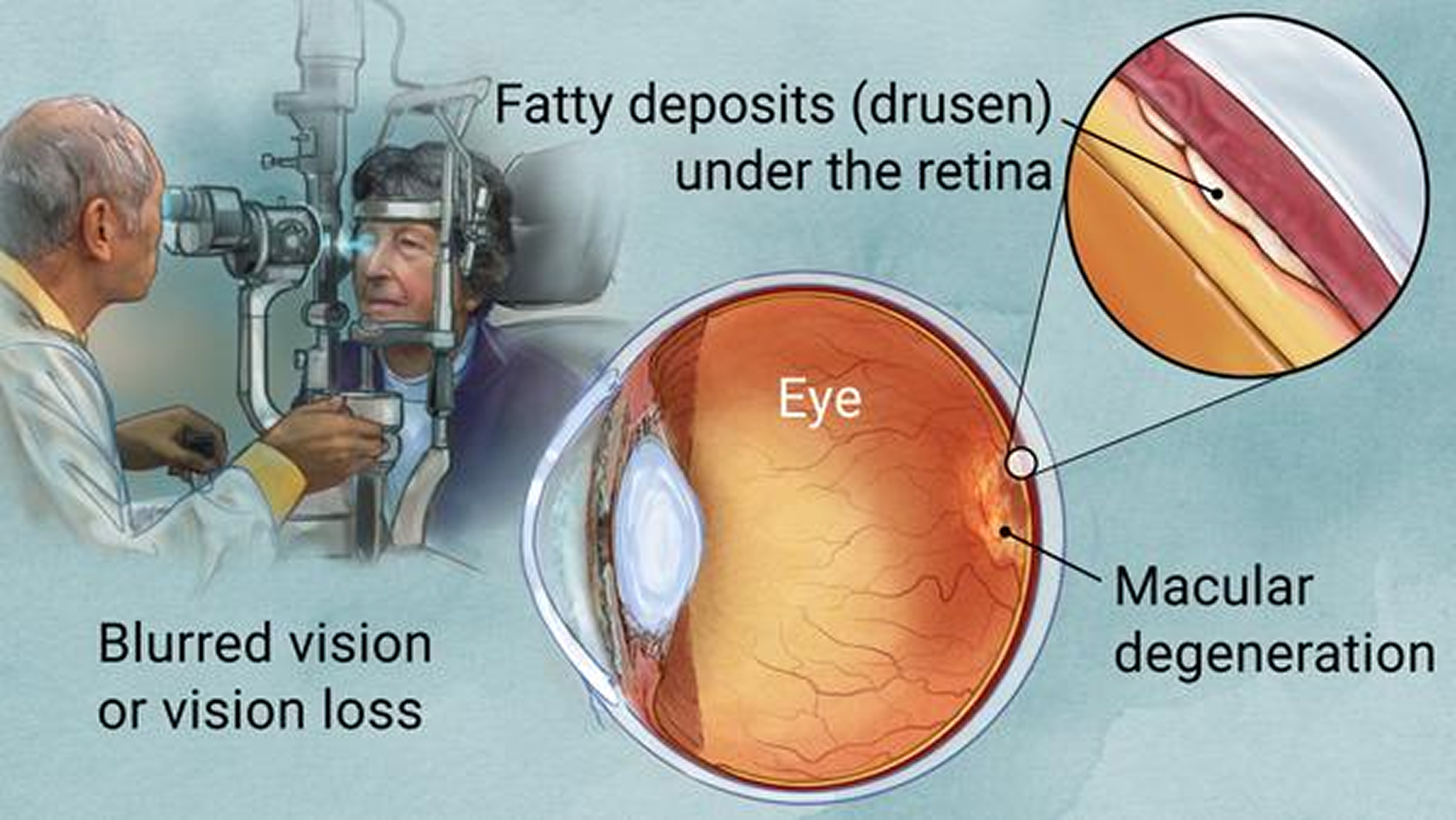
Macular degeneration erodes the macula and central vision, but it’s often a sign of broader circulation, inflammation, and energy imbalances.
Macular dystrophy is a rare genetic disorder that slowly damages the macula, the eye's center for sharp vision, resulting in progressive central vision loss.
Macular edema, also called cystoid macular edema, is swelling in the retina’s center that blurs detail; our goal is early detection & integrative care to help protect sight.
Macular pucker (epiretinal membrane) is a thin scar layer on the macula that contracts, wrinkling the retina and blurring or distorting central vision.
Myopic degeneration is severe nearsightedness that stretches and thins eye tissues, causing progressive vision loss and higher retinal detachment risk.
Pattern dystrophy is an inherited retinal disorder in which pigment collects in distinctive macular patterns, slowly causing central vision to blur.
Wet macular degeneration arises when abnormal retinal blood vessels leak beneath the macula, causing rapid distortion and loss of central vision.