Diabetic Retinopathy
Diabetic retinopathy develops when high blood sugar damages retinal blood vessels, causing blurry vision, floaters, and potentially permanent vision loss.
NAION and retinal occlusion (eye stroke) both cut off blood flow to the eye — one to the optic nerve, the other to the retina. Both demand urgent integrative care to protect and restore vision.
Hear from Dr. Rosenfarb
Whether you prefer hands-on care, convenient telehealth visits, or self-guided learning, we have multiple ways to help you manage NAION / Eye Stroke.

Start here. A member of our care team will review your condition and situation, answer your questions, and walk you through the treatment options that are the best fit for you.
Book your free assessment call
Combining acupuncture, laser therapy & diagnostics at Dr. Rosenfarb's office in New Jersey. 90% of patients see measurable vision improvements.
Learn more
One-on-one virtual sessions with Dr. Rosenfarb. Get personalized assessment and custom treatment plan from home.
Learn more
Scientifically-formulated supplements chosen by Dr. Rosenfarb to nourish your eyes and support healthy vision recovery.
Get supplementsDr. Rosenfarb's top-recommended supplements to nourish and protect your eyes.

Supplements
$65.00

Supplements
$70.00

Vitamins & Supplements
$30.00

Supplements
$30.00$25.00
Save 17%
Ready to take the next step?
Choose whatever feels right for you — no pressure, no commitment.
Common questions we get asked about NAION / Eye Stroke.
NAION is an eye stroke of the optic nerve — blood flow to the front of the optic nerve is cut off, damaging the fibers that carry visual signals to the brain. A retinal occlusion is an eye stroke of the retina — a blocked artery or vein stops circulation to the light-sensing tissue itself. Both cause sudden vision loss and share the same vascular risk factors.
Partial recovery is possible — especially when care begins within weeks. Dr. Rosenfarb often sees field gains after a series of acupuncture, laser, and ACS-3000 sessions.
Treat NAION or eye stroke like any stroke: the sooner circulation and inflammation are addressed, the more cells can be saved. Aim for treatment within the first 4–6 weeks.
Most people never get a second episode, but shared risk factors (sleep apnea, hypertension, diabetes) can endanger the fellow eye. Managing those risks and supporting nerve health lowers the odds.
Yes, but it usually appears in one eye first. Having an occlusion raises the risk of it happening in the fellow eye, so monitoring is crucial.
Mild, non-ischemic cases may regain most visual acuity, especially if treated promptly. Severe ischemic occlusions often leave permanent deficits, though treatment can maximize remaining vision.
They may reduce swelling or bleeding but don't regenerate nerve tissue. Pairing conventional drugs with oxygenation and neuro-stimulation offers a more complete strategy.
EHI prioritizes CBD-rich Catavision for inflammation, Total MA-48 for micro-circulation, neuronal support formulas, high-dose DHA, taurine, and molecular hydrogen for oxidative stress control.
Ideally within hours. Although some therapies can still help days later, early diagnosis and prompt treatment offer the best chance to preserve or restore vision.
Discover other eye conditions that share similar causes, symptoms, or treatment approaches with the one you're exploring.
Diabetic retinopathy develops when high blood sugar damages retinal blood vessels, causing blurry vision, floaters, and potentially permanent vision loss.
Retinal detachment is a medical emergency in which the light-sensitive retina peels away from the eye's back wall, triggering sudden flashes, floaters, and rapid vision loss.
A retinal tear is a small rupture in the eye’s retina that can trigger sudden flashes or floaters and may progress to detachment if untreated.
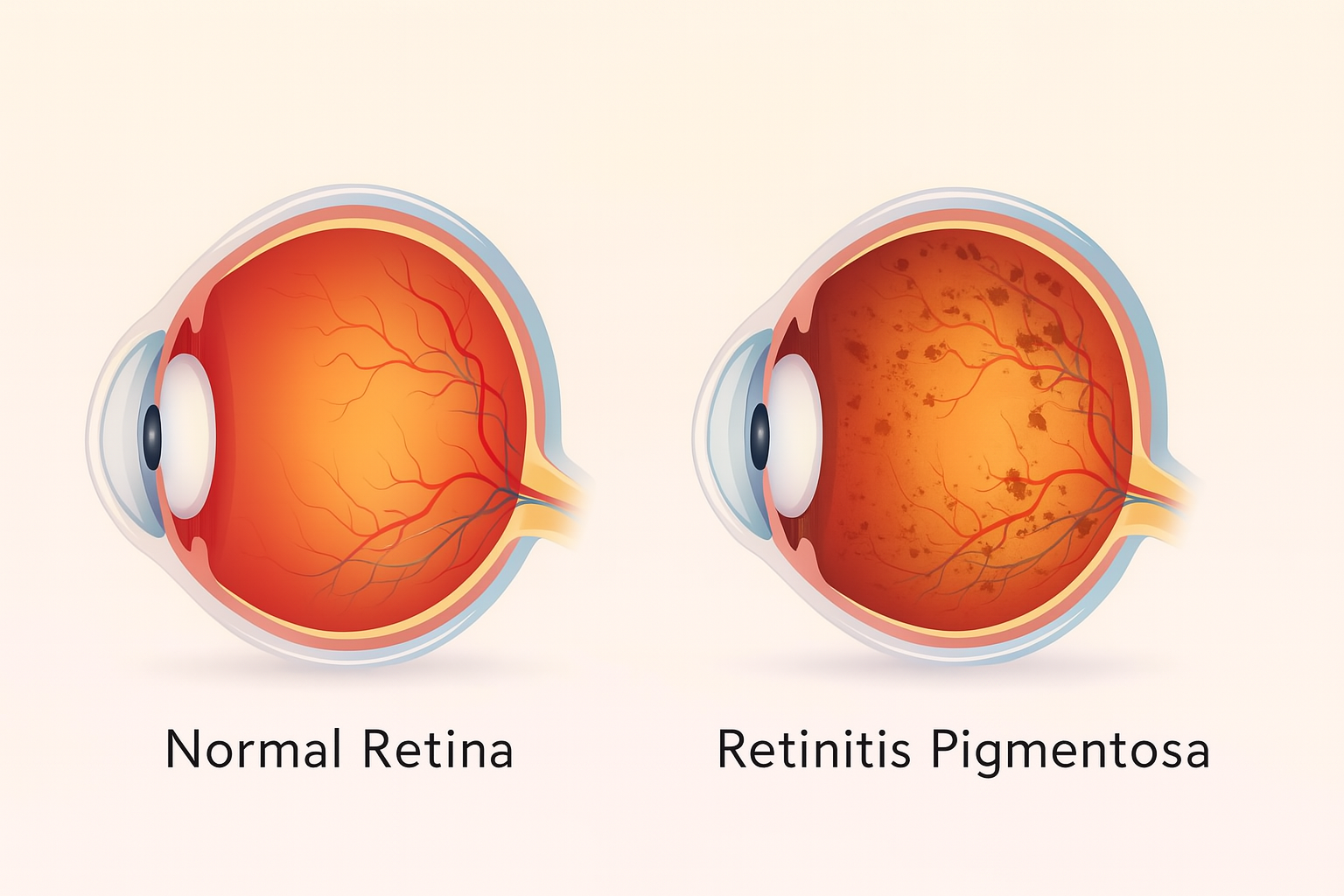
Retinitis pigmentosa is an inherited retinal disorder that gradually destroys photoreceptor cells, leading to night blindness and progressive tunnel vision.