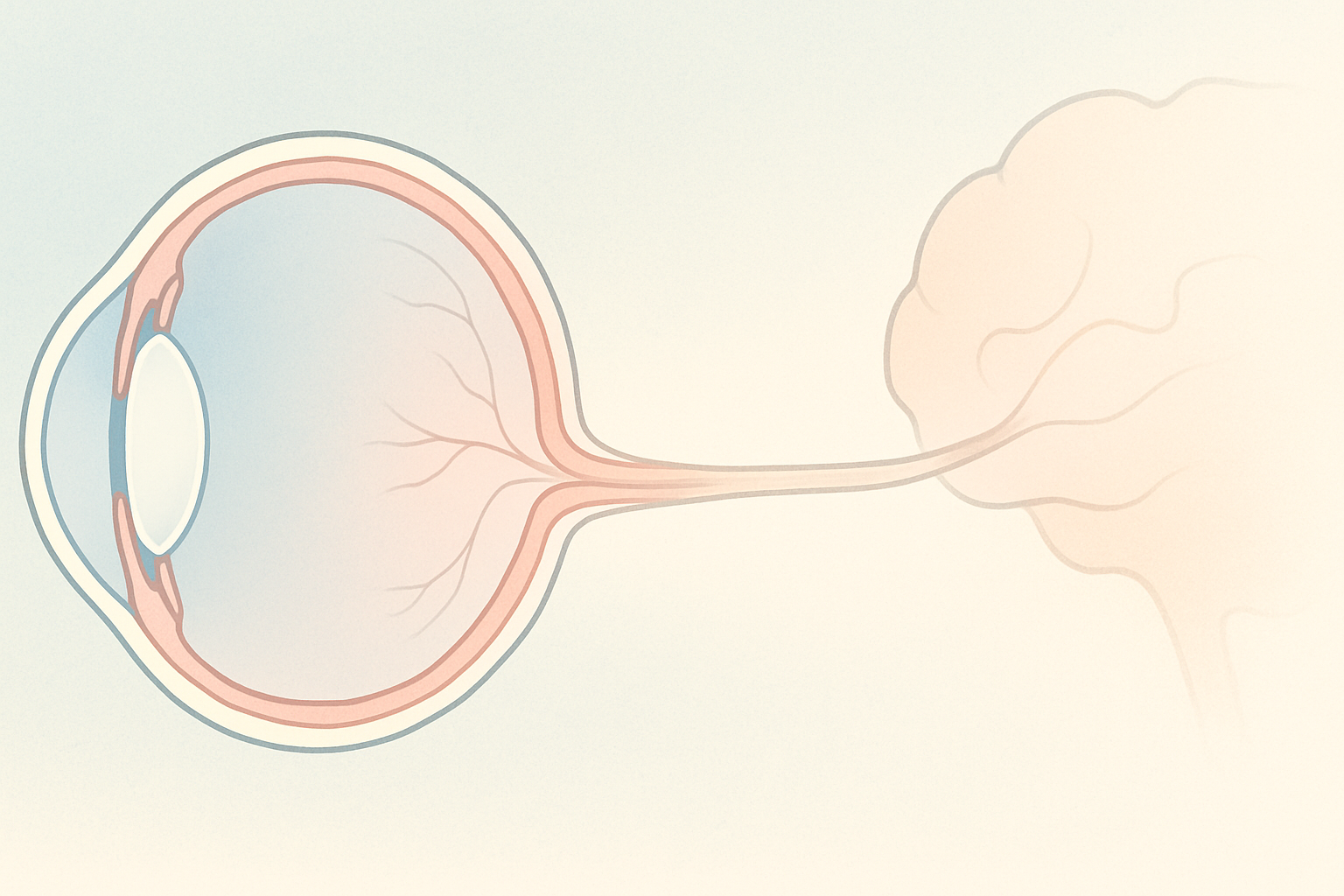
Glaucoma / Optic Nerve
Glaucoma is a group of eye diseases in which elevated eye pressure damages the optic nerve, silently stealing peripheral vision and potentially leading to blindness.
Optic neuritis is an immune-driven inflammation of the optic nerve that can cause sudden vision loss, eye pain, and color desaturation, yet many people recover well with timely, integrative care.
Hear from Dr. Rosenfarb
Whether you prefer hands-on care, convenient telehealth visits, or self-guided learning, we have multiple ways to help you manage Optic Neuritis.

Start here. A member of our care team will review your condition and situation, answer your questions, and walk you through the treatment options that are the best fit for you.
Book your free assessment call
Combining acupuncture, laser therapy & diagnostics at Dr. Rosenfarb's office in New Jersey. 90% of patients see measurable vision improvements.
Learn more
One-on-one virtual sessions with Dr. Rosenfarb. Get personalized assessment and custom treatment plan from home.
Learn more
Scientifically-formulated supplements chosen by Dr. Rosenfarb to nourish your eyes and support healthy vision recovery.
Get supplementsDr. Rosenfarb's top-recommended supplements to nourish and protect your eyes.

Supplements
$65.00

Supplements
$70.00

Vitamins & Supplements
$30.00

Supplements
$30.00$25.00
Save 17%
Ready to take the next step?
Choose whatever feels right for you — no pressure, no commitment.
Common questions we get asked about Optic Neuritis.
No. Optic neuritis is an inflammation of the optic nerve, while MS is a chronic autoimmune disease that can affect many areas of the brain and spinal cord. About half of people who have one episode of optic neuritis eventually develop MS, but many never do. An MRI and blood tests help your neurologist determine the likelihood of MS and whether preventive treatment is needed.
Most people regain 80 – 100 percent of their vision within three to six months, especially if this is their first attack and they receive timely care. Color and contrast sensitivity may lag behind clarity. Repeated or severe episodes can leave permanent blind spots or reduced color vision, so prompt evaluation and follow-up are vital.
Intravenous steroids are standard when vision is severely reduced or if MRI shows extensive inflammation, because they shorten recovery time. However, studies show that final visual acuity is often similar with or without steroids. Your doctor will weigh the benefits against side effects (insomnia, mood changes, elevated blood sugar) and consider alternatives such as plasma exchange for steroid-resistant cases.
It usually starts in one eye, but certain conditions, such as neuromyelitis optica spectrum disorder (NMOSD), MOG-antibody disease, some infections, or toxic exposures, can inflame both optic nerves at once or in quick succession. Sudden vision changes in both eyes warrant immediate emergency evaluation.
Work with your neurologist to manage underlying autoimmune disease, keep vitamin D in the optimal range, avoid smoking, and address infections quickly. An anti-inflammatory diet, regular exercise, stress-reduction practices, and integrative support such as microcurrent and acupuncture at Eye Health Institute may further stabilize immune responses and support nerve health.
Light to moderate activity, such as walking, gentle cycling, or yoga, is generally safe and can improve mood and circulation. Intense heat or vigorous workouts may temporarily worsen vision (“Uhthoff’s phenomenon”), but this is usually reversible. Stay cool, hydrate well, and stop if symptoms flare. Talk to your physician before starting a new routine.
Discover other eye conditions that share similar causes, symptoms, or treatment approaches with the one you're exploring.
Glaucoma is a group of eye diseases in which elevated eye pressure damages the optic nerve, silently stealing peripheral vision and potentially leading to blindness.
Optic nerve atrophy limits the optic nerve’s ability to relay visual signals, leading to progressive vision loss.